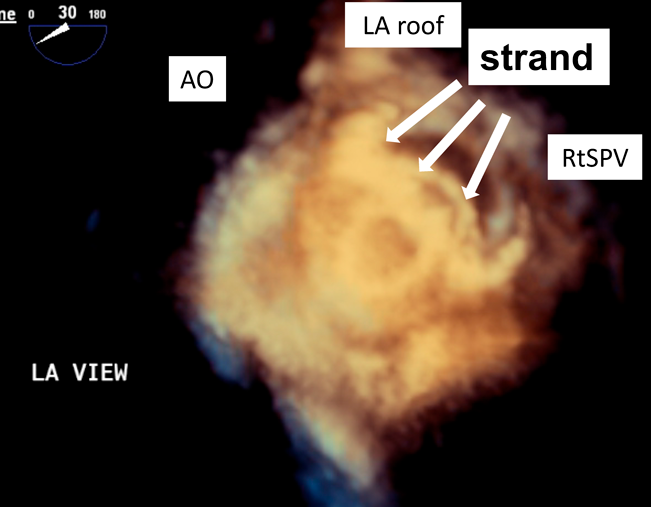
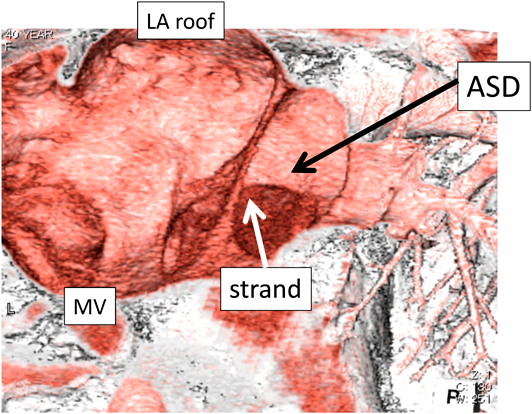
紐状構造物(strand)を支持力の一部として利用した経皮的心房中隔欠損閉鎖術Percutaneous Transcatheter Closure of Atrial Septal Defect Using Strand as a Part of the Supporting Margin
静岡県立こども病院 循環器科Department of Cardiology, Shizuoka Children’s Hospital
受付日:2020年5月27日Received: May 27, 2020
受理日:2021年1月29日Accepted: January 29, 2021
発行日:2021年3月25日Published: March 25, 2021